The rule of trust
Findings from citizens’ juries on the good governance of data in pandemics.
28 July 2022
Reading time: 73 minutes

Executive summary
In July 2021, the Ada Lovelace Institute, working with the University of Edinburgh and the Bingham Centre for the Rule of Law, convened 50 members of the UK public in two online, week-long citizens’ juries.
Developed by the Jefferson Centre in the 1970s, citizens’ juries are a type of structured deliberation with members of the public, sometimes referred to as a ‘mini public’. During facilitated workshops, participants –‘the jurors’ – are given balanced information and expert presentations about a chosen issue, before deliberating on that issue and reaching a conclusion of some kind. The issue usually addresses an area of public policy, and the conclusions generated often take the form of recommendations for policymakers.
During the citizens’ juries convened by Ada, jurors discussed data-driven technologies that played roles in the UK’s response to COVID-19, including vaccine passports, risk-scoring algorithms used to identify clinically vulnerable people, and plans for new health data infrastructures such as the General Practice Data for Planning and Research programme (GPDPR), which intended to share patient data from GP surgeries for use in medical research and central planning.
The jurors were recruited to reflect demographic diversity across the UK, with some overrepresentation of individuals who reported being clinically vulnerable to COVID-19. During the deliberations, jurors considered information about data-driven technologies used during the pandemic, heard from a range of experts and took part in facilitated discussions. They expressed their concerns and suggested criteria for the good governance of data and data-driven technologies.
The jurors were tasked with considering what the good governance of data and technology looks like. During the jurors’ deliberations, Dr Claudia Pagliari of the University of Edinburgh drew on her own and others’ academic research to introduce the concepts underpinning good governance, including their connections to institutional integrity and human rights, and their implications for the use of data and technology during the pandemic. As part of this, she presented a ‘wheel of good governance’ to guide the jurors in their deliberations.
In this report, the Ada Lovelace Institute has synthesised these concepts with the key themes emerging from the citizens juries, and presents seven principles for trustworthy data governance during pandemics:
- Transparency, communication and clarity: there must be clear and consistent communication around the use of data-driven approaches, and application of rules and public health measures during a pandemic.
- Accountability: there must be emphasis on adherence to the rule of law, protecting democracy and ensuring robust, fair and equal enforcement of policies.
- Equity, inclusiveness and non-discrimination: the use of data-driven technologies should not exacerbate unequal social stratification or create a two-tiered society.
- Protection of personal freedoms: use of data-driven technologies should respect and protect individual liberties and rights.
- Proportionate and time-limited uses: data use must balance public health needs and risks to individuals and society, and pandemic response measures must not extend into post-pandemic data futures.
- Emergency preparedness and planning: effective, accurate and responsibly managed data should be the basis for evidence and learning during emergency preparedness and planning.
- Trustworthiness: the organisations and governance structures involved in the design and use of a data-driven technology must be trustworthy.
In addition to trustworthiness being an important principle to guide good governance of data, jurors reflected that public trust in data use is dependent on good data governance. This means that to build public trust and support for data-driven responses to pandemics, establishing good governance according to these seven principles is a foundational step.
Jurors also articulated the following red lines for governance of data-driven technologies in a pandemic:
- Technologies should not create a two-tiered society that disproportionately discriminates against or disadvantages certain groups.
- Any measures exceptionally and temporarily accepted during the pandemic should not be extended into the future, after the pandemic ends.
- Technologies should not be used to surveil, influence, profile or predict the behaviour of individuals.
This report is based on the Ada Lovelace Institute’s analysis of transcripts and notes from the citizens’ juries. Throughout, we share quotes from the transcripts to reflect jurors’ views in their own words. We have edited some quotes for readability, but have not altered their meaning in any way.
The jurors’ deliberations took place at a timely moment during the pandemic. In July 2021, UK Government ministers and officials were indicating support for the implementation of vaccine passports, despite considerable objections from civil society. Health officials were weighing the decision to pause the amidst societal disquiet about its governance. And there was ongoing societal debate across the UK about the appropriate use of patient data in the pandemic and beyond, as well as the appropriate use of algorithms in planning and prioritising access to healthcare.
As we publish this report in summer 2022, with further waves of COVID-19 occurring across the UK and around the world, and with continued focus on the use of health data exemplified through the publication of several health data strategies and policies, these topics remain pertinent and the juries’ findings remain relevant.
Introduction
Data has played a vital role in the UK’s public health response to COVID-19. It has taken centre stage through charts and dashboards seen in press briefings, enabled the development of apps such as contact tracing and vaccine passports, powered risk-scoring algorithms that identify those most vulnerable, underpinned medical treatment and research infrastructure, and much more. Data is critical to addressing the pandemic, and will remain so throughout the remainder of the COVID-19 crisis and into any future pandemics the world may face.
However, in a national emergency, data-driven approaches may often correlate with the curtailing of personal and social liberties, and require public compliance with new technologies and health measures such as digital contact tracing and social distancing. It is vital that data-driven technologies and approaches are implemented in ways that the public can trust and have confidence in. The good governance of data and effective application of the rule of law are crucial to ensuring that trust and confidence.
In 2021 the Arts and Humanities Research Council, as part of the UK Research and Innovation rapid response to COVID-19, funded a group of researchers led by the Bingham Centre for the Rule of Law, part of the British Institute of International and Comparative Law (BIICL), to conduct research into the role of good governance, and the rule of law in building public trust in data-driven responses to public health emergencies. The project team included researchers from BIICL, the Universities of Edinburgh and Newcastle, the Alan Turing Institute and the Ada Lovelace Institute.
As part of this project, the Ada Lovelace Institute coordinated two citizens’ juries in July 2021. 50 participants from across the UK took part in the juries over the course of two online, week-long deliberations. These ‘jurors’ listened to expert testimonies and considered information about the use of data-driven technologies and data infrastructures in the COVID-19 response.
The jurors explored several case studies of technologies and data infrastructures, including plans for future health data infrastructures such as the General Practice Data for Planning and Research (GPDPR) programme for collecting patient data from GP surgeries for use in medical research and central planning, vaccine passports and risk-scoring algorithms used to prioritise vaccinations and identify clinically vulnerable people. They were tasked with addressing two interconnected questions:
- What constitutes good governance of data-driven technologies?
- What constitutes proportionate uses of data-driven technologies during pandemics?
While jurors recognised the importance of taking urgent and significant action to address and respond to the pandemic, including using data-driven technologies, they were also critical of how some measures were implemented.
Jurors were concerned about the impact of some data-driven technologies, such as contact tracing and vaccine passports, on civil liberties and public surveillance. They highlighted a perceived lack of transparency, accountability and communication in the use of data, and were uncertain about the trustworthiness of the institutions managing and using the data, particularly commercial companies. Jurors were also critical of ‘app-based responses’ that divert attention from investing in the healthcare infrastructure, and the lack of public health coordination.
At the heart of these critiques, jurors underlined the need for transparent, accountable and inclusive pandemic responses that are developed, implemented and revised by trustworthy institutions and actors. The findings of these citizens’ juries include a set of seven principles and three red lines for the good governance of data during pandemics.
This report is based on the Ada Lovelace Institute’s analysis of transcripts and notes from the citizens’ juries. Throughout, we share quotes from the transcripts to reflect jurors’ views in their own words. We have edited some quotes for readability, but have not altered their meaning in any way.
Findings: Seven principles for trustworthy data governance in pandemics
During the deliberations, jurors considered a model of good governance presented to them by Dr Claudia Pagliari: ‘the wheel of good governance’ as shown in figure 1.
Figure 1: The wheel of good governance presented to jurors.1
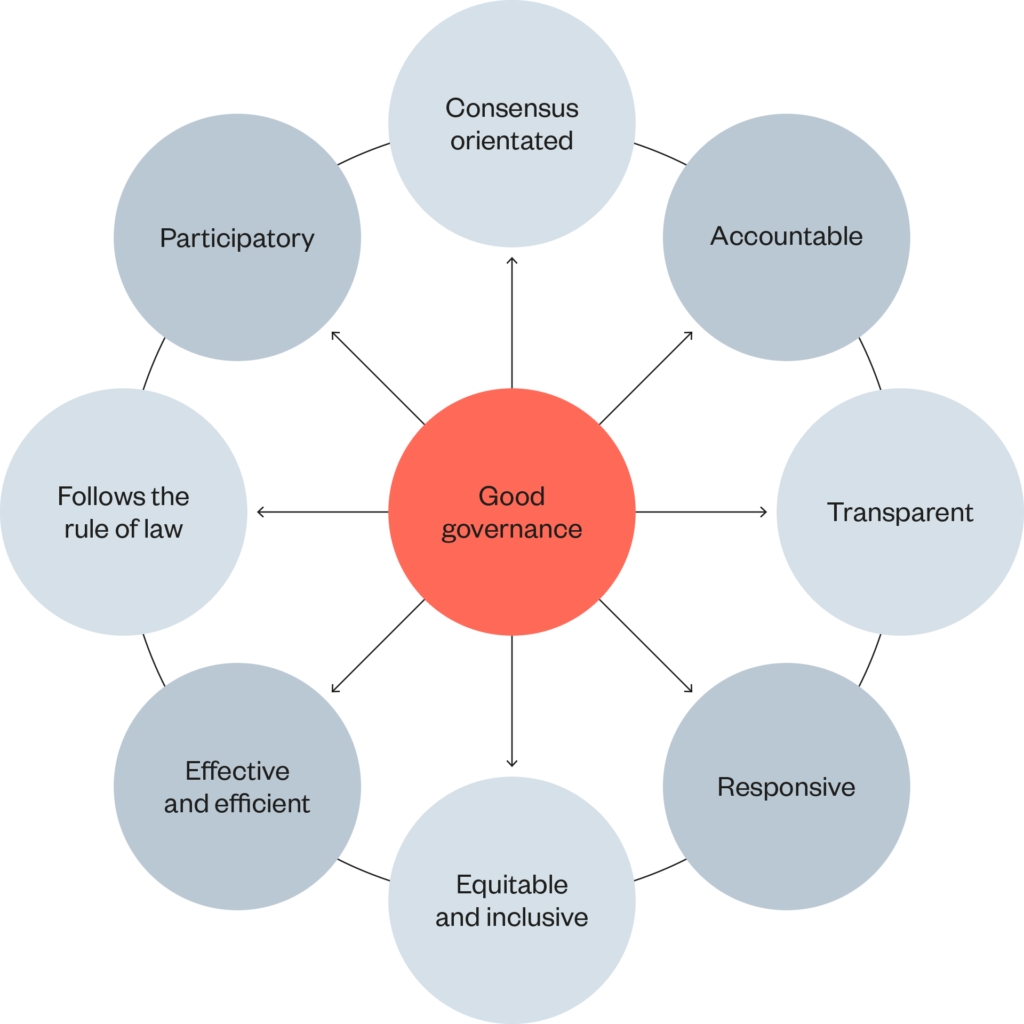
From this, the jurors questioned and considered how they might define the principles of good governance of data and data-driven technologies during pandemics.
Below, we describe the jurors’ deliberations according to themes that emerged from their discussions. These themes inform a set of seven principles for good data governance during pandemics:
Figure 2: Seven principles for good data governance
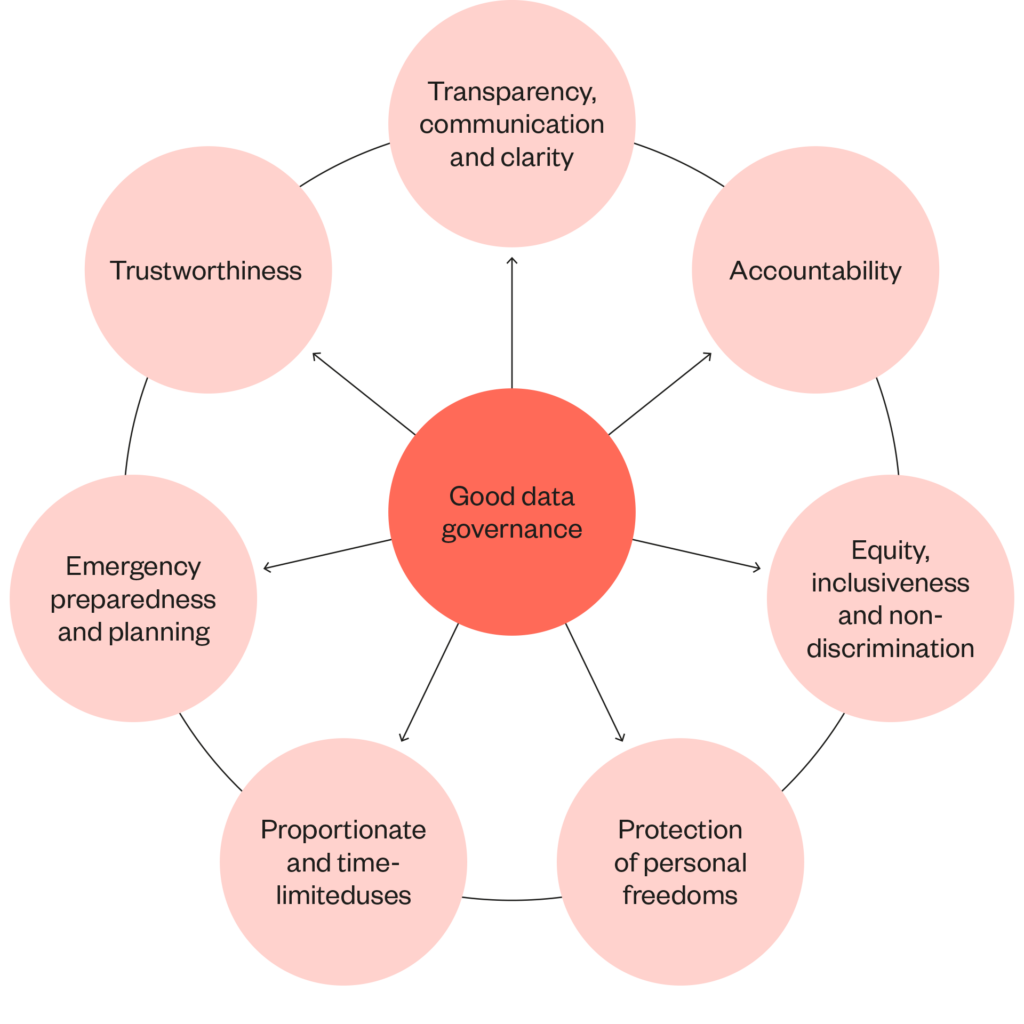
- Transparency, communication and clarity
- Accountability
- Equity, inclusiveness and non-discrimination
- Protection of personal freedoms
- Proportionate and time-limited uses
- Emergency preparedness and planning
- Trustworthiness
1. Transparency, communication and clarity
Jurors often indicated the importance of consistency and clarity about lockdown rules and more simplified communication during the pandemic:
‘All of those different messages all of the time, it allows people to have the excuse to not do things because they can say it’s not clear.’
‘Transparency, clearer rules. That’s one of the important [missing principles] that led on to the people at the top being able to bend the rules to suit themselves.’
Referring specifically to data use, participants emphasised the importance of transparency and clarity about the precise use and purpose of data collection and management. Where data is being used, gathered or accessed, they called for increased transparency about what data is involved, the purpose for which it is being used and a clear explanation of the relevant safeguards and data protections in place. Jurors put particular emphasis on transparency when discussing the General Practice Data for Planning and Research (GPDPR) programme, even though they acknowledged that there were potentially beneficial uses of that data, for instance to help advance medical research.
Some of the jurors also indicated that only informing people about what happens to data is often insufficient. Where a person is individually affected by data, jurors felt it was important that they had adequate choice and control over its use, and saw this as an extension of transparency itself.
‘Transparency by means of understanding the parameters of these technologies, why we need them and what our rights are.’
The jurors identified an overlap between transparency and accountability mechanisms, and wanted greater clarity about accountability and the relevant checks and balances in place. This was particularly important where they perceived a risk that established accountability mechanisms may be eroded during the pandemic, and led to jurors’ expectations for transparency in a crisis overlapping with those for accountability.
‘There is no accountability for these businesses or scientific bodies because it’s a state of emergency. My fear would be that we might end up in a constant pandemic because there is no accountability.’
2. Accountability
Jurors identified three components to ensuring Government-led responses to the pandemic are accountable: rules applied without exceptions; a fair distribution of responsibility across government, public institutions and members of the public themselves; and open and scrutable decision-making.
‘It is a kind of “one rule for us, one rule for them” kind of mentality and I thought that was grey throughout the pandemic.’
Jurors reflected on the close scrutiny placed on the UK Government following incidents where key officials had violated public health restrictions.2 This was prominent in discussions about digital contact tracing, where jurors said that the perception that ministers and officials were not adhering to lockdown rules undermined public confidence in the collective effort to address the public health challenge of the pandemic.
One example of this, cited by jurors, was Dominic Cummings’ alleged visit to Barnard Castle during lockdown, while he was a key Cabinet Office aide.3
‘Look at Dominic Cummings … You have to practice what you preach, have clear communications and set it up in a way that people can access equally.’
Jurors were uneasy about the double standard such violations created, and felt the apparent willingness among Government officials to disregard the rule of law was a result of them not being held to account.
Jurors reflected on how Government officials – whether elected or staff – are regarded as norm-setters. When those officials contradict the public health advice and restrictions they decided to enforce, citizens are less likely to accept the legitimacy of these restrictions. The jurors felt these double standards undermined the public trust required for widespread compliance with public health measures, and encouraged members of the public to make their own moral judgement calls as to the appropriateness of actions, rather than follow a consistent approach led by public bodies.
‘Why am I listening to people who are breaking the law that they are putting in place? I think they can break the law because they are going to get away with it.’
‘Instead of relying on the rule of law for everyone, it is your own moral compass and what you deem the right way to behave. I care more about society than myself and I believe it’s important for me to do what’s right for everyone and to protect everyone as much as I can. Whereas members of Government don’t really seem to have the same opinion, because they have a different moral compass.’
Events relating to senior policymakers in Number 10 hosting parties during the lockdown in 2020 have further highlighted the importance of trustworthy actors and institutions to the overall trust in the pandemic response.4 Such incidents further demonstrate how actions that undermine the confidence in institutions tasked with leading the pandemic response diminish trust in the overall system, including the data-driven interventions deployed.
The responsibilities of government, public bodies and individuals in addressing the pandemic should be balanced fairly
Jurors felt that the Government, not individuals, are responsible for managing risks associated with responding to a public health emergency. However, jurors noted how reliance on technology interventions can shift the burden of responsibility for managing the pandemic from the Government to individuals. This phenomenon is often described as ‘responsibilisation’.5
Jurors discussed how some data-driven responses to COVID-19 have shifted the burden of responsibility to individuals. These shifts ranged from requirements to download apps and respond to notifications, to verifying their COVID-19 status prior to entry to public spaces.
Although some jurors felt that individuals should take some responsibility for managing their behaviour during the pandemic, they were critical of overreliance on technological solutions that reduce governmental responsibility and felt the need for legal checks and balances to mitigate this.
‘Having a legal requirement would hold the Government to account by the Opposition and by the public as well. We thought it would reduce blame culture because the responsibility would be held by the Government rather than the public or companies or people having to enforce these things.’
Decision-making processes should be open, inclusive and subject to public scrutiny
‘Right now, I feel we should come up with solutions between the Government, legal professionals, health professionals and us.’
Jurors recommended creating an independent body that brings together policy professionals, decision-makers, a range of experts and members of the public to hold data-driven technologies accountable. This resembled a previous proposal made by the Ada Lovelace Institute: the Group of Advisors on Technology in Emergencies (GATE).6 While the jurors were not introduced to the idea of GATE during their deliberations, the fact that they independently drew similar conclusions demonstrates the strength of need for an independent body, inclusive of lay members, to support the governance of data-driven technologies during pandemics.
Jurors were concerned that the immediacy of the pandemic crisis response meant only a relatively narrow range of perspectives, interests and experiences could be considered. This highlights a need to adapt, iterate and strengthen inclusive decision-making processes rather than erode them at times of crisis. In the long term, policymakers may wish to consider institutionalising public engagement and accountability mechanisms7 for assessing data-driven technologies that may be used in future pandemics:
‘For me good governance might be a place where citizens […] have a democratic parliament of technology, something to hold scrutiny.’
3. Equity, inclusiveness and non-discrimination
‘I think we probably have created a two-tier society with Track and Trace [sic] in that it’s easy for people like myself who can work from home. If I was a taxi driver, worked in retail, had a job that couldn’t be done from home – would I self-isolate if I was pinged? […] I probably wouldn’t have the app if I’m truly honest. Because how would I put food on the table when a lot of the Government subsidies were taken away when the lockdown was lifted?’
Jurors identified how some data-driven interventions risk creating a ‘two-tiered society’, and expressed concern about the onward effect of who benefits from, contributes to, and has public confidence in data-driven technologies. Their deliberations covered three risks of technology development during a pandemic that may contribute towards the creation of a ‘two-tiered society’.
Firstly, jurors questioned the assumption that technologies will be experienced equally by people. In the case of digital contact tracing, jurors noted how the assumption was made that everyone can isolate and stay at home while also maintaining their sources of income. For vaccine passports, jurors challenged the assumption that everyone can use a smartphone to demonstrate their vaccination status. Jurors discussed the risk these interventions posed to exacerbate pre-existing socio-economic disadvantage and social inequalities arising from the pandemic:
‘I’m very fortunate I can work from home, I’m a single parent. If I was the kind of person who had to go out to work, yes, it would affect my decisions. If there’s one income coming into the house, I feel sorry for people. It’s very, very difficult. Very difficult if you need to put food on the table. I wouldn’t judge anyone in those circumstances.’
Jurors also identified that public health advice to isolate until no longer infectious or at-risk only works for people who do not share a house. They noted how, in reality, many people live in shared housing or have no fixed address, making compliance with the notification and advice nearly impossible:
‘Why should we waste our time isolating for ten days, potentially losing out on money? For someone living pay cheque to pay cheque, you can’t afford to say, “sorry, I can’t come into work for ten days” when it doesn’t make sense and the rest of your family can go out even though you’re in the same house.’
Secondly, jurors critiqued the assumption that there is equal access to digital infrastructure, such as reliable internet connection or devices, or having the relevant skills to use the technologies effectively.8
They thought that contact tracing apps risked furthering societal inequality, as a significant proportion of the UK public lack access to either a smartphone or broadband, and there are differences in the skills, confidence and capabilities needed to use such technologies:
‘There are huge parts of the population potentially left out, for instance, the elderly with no smartphones.’
‘What about the homeless who don’t have a smartphone? What about the people who have old phones, like my mother?’
There were also concerns about how centralised, digital-by-default approaches could displace on the ground, localised, targeted interventions which might have a better and more direct understanding of communities’ immediate needs.
Thirdly, jurors shared concerns about the risk of data being used for surveillance, with discriminatory consequences. They considered whether data collected during the pandemic could be used to profile or target particular groups, such as those as having greater COVID-19 vulnerability, being subject to increased profiling and data collection than those who are not. They also considered the risk that individuals’ vaccine statuses could be used in harmful or unfair ways. Participants observed how data-driven interventions could mean that the link between health inequalities and social inequalities is exacerbated:
‘There’s a whole other kind of distinction between two levels of society: people who have got the time and the money to access healthy foods and healthy lifestyles and people who don’t. And it’s not people’s fault if they can’t access that.’
The jurors felt that the blanket roll out of technology solutions has implications on the lives of individuals which are mostly unaccounted for in the development, implementation or, evaluation phases of a technological solution’s lifespan.
The jurors concluded that good governance of data-driven technologies during a pandemic must include a holistic understanding of the complex and nuanced ways in which inequities and discrimination can be perpetuated through the use of data. They placed a strong emphasis on hybrid approaches that include non-digital measures to ensure that public interventions account for everyone’s needs and circumstances.
The data divide
The adoption of data-driven technologies can create unequal impacts due to inequities in the way that data is used and gathered, inequities in who the technologies are designed for, as well as inequities in how people experience (either directly or indirectly) the technologies.
Through a survey conducted in early 2021, the Ada Lovelace Institute identified and described a ‘data divide’: inequalities in who is included or excluded from datasets that underpin technological interventions in health.9 This divide is intertwined with the ‘digital divide’, which describes the different outcomes for those who do or do not have the means, access and capabilities to use digital technologies.
The combination of data and digital divides has an onward effect on who can be represented by, and has agency to shape, data-driven technologies. COVID-19 technologies, such as digital contact tracing, risk scoring and vaccine passports, are no exception to this general rule.
4. Protection of personal freedoms
‘We should have ownership and agency over our own digital identity. Is there a power grab here?’
A dominant theme in the jurors’ discussions, particularly in relation to vaccine passports and digital contact tracing, was the extent to which COVID-19 technologies challenged individual freedoms and liberties.
To some extent, these discussions were framed in relation to privacy as a right, and one that must not be easily ‘lost in a hurry’, as one juror described it. However, concerns about personal liberties also extended towards the normalisation of surveillance through data:
‘Ten years down the line, a private insurance company could know my grandparents died of cancer and refuse treatment on the basis of that.’
Jurors discussed the risk that the accelerating adoption of technologies may lead to wider adoption of behavioural science approaches that nudge, shape and influence individual behaviour, a concern raised particularly in the context of vaccine passports. Jurors wondered whether the implementation of vaccine passports would undermine people’s freedom of choice around taking a vaccine, and expressed that people should not be penalised for a personal choice. However, not all jurors were opposed to vaccine passports on these grounds. One of the most cited benefits of vaccine passports was the extent to which their implementation might incentivise vaccine uptake, hastening a return to society as normal.
Jurors expected to see pandemic governance of data-driven systems anticipating and safeguarding effectively against the risks of surveillance and tracking – as well as recognising the potential asymmetries of power, agency and control between the data subject and those involved in data collection, use and sharing.
5. Proportionate and time-limited uses
In dialogue with experts, jurors considered two approaches to proportionality which are informed by legal traditions. The first approach considers the balance between the restrictions imposed by a measure and the severity of the prohibited act. The second approach considers the extent to which Government measures are proportionate to the purpose of those measures.
The theme of ‘checks and balances’ dominated these discussions, and there was considerable scepticism among jurors about the extent to which they prevailed during a pandemic:
‘There are no checks and balances going on. It is an emergency so they can do whatever they want.’
Jurors were especially wary about the potential consequences of loose and vague data protection legal frameworks that could govern data managed in the proposed GPDPR. In particular, they were concerned about how the legal frameworks may be interpreted in a manner that meant any imminent need would justify the collection and processing of data without clarification of personal data protection frameworks. Such measures were perceived to bypass key democratic checks and balances – such as transparency – that should be embedded in data governance.
Despite this scepticism, jurors also recognised the importance of a response that was both rapid but also balanced and proportionate during the pandemic. For example, some jurors shared that they had taken part in data donation programmes such as the ZOE app.10
Others identified the value of using data to generate real-time, precise information to inform pandemic planning, as well as ensuring benefits to medical research on COVID-19 were realised.
In addition to their recognition of these numerous potential benefits, jurors stressed that data, in isolation, was not a panacea. They questioned whether overreliance on data-driven interventions was proportionate, and placed emphasis on a balanced approach that recognised how data use must be complemented by person- and community-centred approaches that can understand the limits to how well data can reflect the full realities of people’s lived experiences of the pandemic.
In considering the range of use cases, jurors emphasised how some uses would be tenable and justified only in an emergency and not beyond. As a consequence, jurors placed a strong emphasis on considering the potential for novel and exceptional interventions to become ‘normalised’ or embedded inadvertently as part of future data infrastructures:
‘But in the future, the life you save is potentially going to be ruined through the means that [governments and private companies] use the data. It is not a win-win situation because you don’t know where you stand because you can’t even measure the damage that it’s going to do in the future.’
6. Emergency preparedness and planning
Jurors took a pragmatic approach and raised questions about the effectiveness and the efficacy of data-driven technologies and interventions. They identified the importance of measuring the impact of data-driven technologies to help inform public health responses throughout the COVID-19 crisis and in future pandemics.
Jurors questioned whether the comparative cost and time involved in developing novel data-driven systems was justified, or whether it might have been more appropriate to resource other mechanisms, recognising the limited resources at policymakers’ disposal and the urgency of the pandemic.
They also sought measures and mechanisms that enabled society at large to better understand some of the key lessons to be learned from such interventions, and emphasised the importance of public involvement in measures such as evaluations and audits of technologies:
‘We can bring in qualitative points and get into the nuances of gaps in understanding around why certain communities are suffering more than others over time, in preparedness for whatever comes next.’
Jurors also emphasised the importance of investing in foresight and forward planning mechanisms, to enable preparedness for future emergencies and pandemics. They felt this was crucial to preventing the need to duplicate work that had already been undertaken, and to prevent the loss of learnings from this pandemic.
‘There are checks and balances, there is consistency because things are in place for future proofing, hopefully. But secondly, if something goes wrong, remove it, correct it and that would solve a lot of problems we have now.’
7. Trustworthiness
Trust was one of the most prominent topics throughout the juries, running through almost all of the jurors’ deliberations. Jurors’ discussions indicated that trust is both a byproduct and a component of good governance. In other words, while good governance is crucial to enabling the public to trust data governance, the good governance of data-driven responses to a crisis depends on the extent to which the data, technologies, actors and institutions in the system are deemed to be trustworthy.
The connection between trust in data-driven technologies and the trustworthiness of related actors and institutions has been evidenced in an extensive body of research. This work shows that trust in data-driven technologies is dependent on how trustworthy those involved in collecting and using data are, including technology developers, charities, health service officials, policymakers, politicians and regulators.11
Jurors’ thoughts on trustworthy data use echoed this. They considered trust in data-driven technologies as contingent on the trustworthiness of:
- institutions tasked and entrusted with leading the pandemic response
- developers who build data-driven technologies
- the technologies themselves
- data governance frameworks.
Trustworthiness of government, public institutions, technology developers and the private sector
‘When the [contact tracing] app came out, I downloaded it. I wasn’t going anywhere, so it never pinged me. In recent months, with all these MPs and people in Government just breaking the rules, and absolutely no accountability, it makes you think “why am I doing it?” […] I can’t help thinking if the NHS was running the pandemic, the NHS was making the decisions, a lot more people would follow the rules and would feel happier, safer.’
Jurors felt varied levels of trust in the different organisations and institutions involved in leading the pandemic response. Some were more willing to trust institutions such as the NHS, medical officers and local coordinating bodies on the front line of the pandemic response (such as local authorities responding to immediate needs), but they expressed greater scepticism about politicians, civil service bodies and the private sector.
In particular, jurors raised concerns about how services to respond to the pandemic – such as acquiring personal protective equipment – were procured. They questioned whether the UK Government’s approach to procurement was trustworthy, especially during the pandemic emergency. Jurors recognised the supportive role of the private sector, but expressed criticism of how appropriate tendering processes had been bypassed due to financial constraints and the need to act fast. In terms of data-driven technologies, they felt this approach posed risks for the standards, effectiveness and quality of these interventions:
‘Because budgets are being driven down for these things, [governments] have to just go to private companies, and then you end up with companies that maybe don’t have the expertise to deal with certain things. At the time it’s rubbish tendering process [and] it feels like it is happening behind closed doors.’
Jurors commented on the role of the private sector in providing services in the pandemic response, from manufacturing personal protective equipment and running testing centres, to designing and developing data-driven technologies like contact tracing apps and decision-making dashboards. They expressed that there was a tension between the focus on public benefit at a time of emergency, and the commercial incentives and the governance structures of technology developers in the private sector, whose primary duty is to maximise benefits and profit for their shareholders. Jurors offered several examples where they felt that private companies and the Government together did not demonstrate their trustworthiness:
‘The mistrust comes from not just the Government but […] the people who handle our data and the ways they handle our data. We are just like pawns for profit.’
‘Seeing how Serco, with Track and Trace [sic] they got the contract very quickly, it was rolled out very quickly. […] It makes me a bit mistrusting.’12
Jurors’ other anxieties related to profit incentives being misaligned with the incentives to take a more thoughtful, considered approach to getting data and technology right. They were concerned this would lead to moving quickly in a ‘DIY’ fashion instead of delivering a higher quality data-driven response.
There were also concerns that commercial companies might abuse their position and exploit public bodies in need of immediate support at a time of emergency, contributing to ‘backdoor privatisation’ of the NHS. Jurors consequently placed a strong emphasis on the need to ensure that there were restrictions to prevent the sale and commodification of data.
Trustworthiness of technology itself: it is no silver bullet
‘“Use data, use the tech to fix the problem.” I think that’s very indicative of where we’re at as a society at the moment […] I don’t think that’s a good modality for society. I don’t think we’re going down a good road with that.’
Jurors were cautious about approaches that positioned new data-driven technologies as a silver bullet but failed to respond to existing, typically non-technological problems.
For instance, jurors felt that supporting those on the lowest incomes during lockdown requires targeted social intervention informed by engagement with affected communities, not poorly thought-through apps or other digital interventions. Jurors expressed concern about what implicit assumptions underpinned the development of technologies, for instance, assuming that an app or digital tool will work for all individuals, regardless of diversity in lived experience:
‘The technology does make our life easier [but] when it comes to person to person, it does vary. Everyone’s situation and condition is different.’
Other critiques addressed the extent to which the technologies had delivered on their promise to help address the impact of the pandemic. In some situations, jurors expressed that trust in data-driven technologies is low because they have been shown to be ineffective and unreliable, as with the use of digital contact tracing:
‘If [digital contact tracing] was a fully working system that made complete and utter sense, then I’d think people would be more likely to go for it.’
For many jurors, the UK contact tracing app was not delivering on its promised purpose. Multiple errors in its use and application, particularly during the earlier stages of roll out, impacted on how likely people were to continue to download, use, and rely on the app:
‘I’ve seen errors happen on the Track and Trace [sic] app. [People have] had messages later on saying, “That was an error”. How do you trust it?.’
‘My next-door neighbour had COVID during the pandemic […] If [the contact tracing app] was efficient, [it] would have notified me about the next-door neighbour. Both my wife and I received no information. I’m a bit flummoxed about how good the technology is.’
Participants also underlined that trustworthy technology is one whose design, use and evaluation accommodates different users and their varied needs. In other words, a trustworthy technology should be effective and fit-for-purpose for all individuals, and not exclude any particular groups. Based on this, jurors emphasised acknowledging people’s lived experiences in technology design and use, taking a ‘bottom-up’ approach that starts from people’s needs and at an individual rather than societal level. In the following quote, one juror expresses this consideration using the example of the efficacy of contact tracing apps:
‘Is contact tracing going to work effectively for us all to have a mutual and shared faith in it doing its job properly?’
Some jurors drew a more direct connection between their trust and confidence in the technologies and their trust in the actors involved in developing and deploying them. This illustrates the extent to which trust in technologies depends on trust in the actors in the overall system:
‘I don’t trust the technologies […] because they have been put together so quickly by companies that are doing it for a profit. How do you trust it to work correctly in the future or anything else that the Government puts out to us or promotes to us to use as a control during the pandemic?’
Trustworthiness of data governance models
In their deliberations, jurors considered how the quality and reliability of data infrastructures and governance models affect public confidence in data collection, access and processing practices.
A key case study jurors discussed in relation to this was the General Practice Data for Planning and Research (GPDPR) programme.13 This programme was intended to update NHS processes for collecting patient data from GP surgeries for use in medical research and central planning. Due to be implemented in September 2021, at the time of the juries it had been paused to allow for further consultation with GPs and patients, following considerable public outcry from patient groups, journalists, campaigners and doctors.
Discussing GPDPR during the midst of this outcry, jurors raised questions about the relevance of GPDPR data for a pandemic when that data may be outdated or collected for a different purpose entirely. While access to high quality, real-time data supported the pandemic response, jurors questioned the necessity and proportionality of data use, as well as purpose limitation for emergency data use. Jurors’ comments suggested that unnecessary and disproportionate data collection are signals of poor and untrustworthy data governance:
‘I would want really clear reassurance from the Government that [the data was] used solely for that purpose and what the timeframe was.’
Concerns about the trustworthiness of the GPDPR were a core part of the broader public discourse, with increased opt-outs from the scheme and public backlash contributing to the ultimate postponement of the programme.14
Jurors’ expectations for trustworthy governance of data during pandemics included time limits on the restrictions of rights, freedoms and accountability. They highlighted any compromises made on these issues as exceptional, and expressed concern about potential for such compromises to become normalised in ‘post-pandemic’ futures. When deliberating algorithmic risk-scoring for example, jurors recognised its usefulness during the pandemic, but noted a high risk that such tools could be misused post-pandemic. For the jurors, this risk warranted strict implementation of a time limit on its use:
‘Once everybody has been vaccinated, there’s no need for [risk scoring] because the whole point of it was to collate all of this information to see who needed it most immediately. Once everybody has been done, that’s invalid.’
Jurors’ concerns about limits of the role of data-driven interventions applied to other technologies too, including vaccine passports based on people’s identities. Here jurors considered the potential for scope creep in the form of personal data being misappropriated or misused to create digital identities. Jurors distinguished between paper-based identity methods and digital identity methods on the basis that the potential for abuse and misappropriation is far more limited for paper records than digital records:
‘If it was on paper, or a card or whatever, it would only serve one purpose, be a COVID card, like a yellow fever card or something like that. They can’t use your data for anything else.’
The jurors’ concerns here centred on the possibility that data governance infrastructures used for legitimate or acceptable purposes might be subject to scope
creep or affected by wider political or social changes (for instance, a change in the democratic nature of a government that further eroded citizens’ rights). To some extent, trustworthiness of data governance was also contingent on the trustworthiness of a government, but jurors were keen to stress the importance of recognising the potential for unintended consequences:
‘It is the risk of abusing data which I am worried about. If all of these things were basically independent from the political environment, [it wouldn’t] depend on who is there at that point, if it’s a fascist government or a more liberal government.’
Data-driven systems considered during the citizens’ juries
During their deliberations, jurors considered several data-driven systems: digital contact tracing apps; risk-scoring algorithms that identified people vulnerable to COVID-19; vaccine passports; and the General Practice Data for Planning and Research scheme (GPDPR). Jurors identified vaccine passports, risk-scoring algorithms and the GPDPR as case studies of particular interest, and heard from subject matter experts to learn more about these systems.
These case studies supported the jurors’ discussions about good governance of data during pandemics, and informed the seven principles detailed above. In addition, the jurors considered the benefits, risks and conditions for the good governance of each case study, detailed below.
Health data sharing in pandemics: the GPDPR
In May 2021, NHS Digital announced a new primary care data collection service, called the GPDPR programme.15
The GPDPR would replace existing decentralised systems for collecting, storing and processing personal health data, by bringing pseudonymised and encrypted data from GP practices throughout England to a centralised system accessible to clinicians, academics, researchers, charities and commercial organisations.16 Its intended aims were to support healthcare planning and research, with the potential for identifying vulnerable groups and pressing healthcare needs.17
However, despite support for the GPDPR’s potential to better manage and link data during the pandemic, concerns grew around data management and governance, and whether patients had been appropriately informed and given opportunities to consent. As a consequence, in June 2021 the proposal to implement GPDPR was delayed, and the implementation date for September 2021 was scrapped.18
The GPDPR programme offered jurors an opportunity to consider the governance of a health data management scheme, in the live context of the ongoing pandemic and as developments occurred.
Below, we summarise jurors’ perspectives on the benefits, risks, and conditions for good governance of GPDPR.
Benefits of the GPDPR
‘If we had a huge NHS database where all the information is fed to a database, a centralised place, life would have been so much easier in the pandemic.’
‘It’s the lack of trust that makes you worry what is going to happen to the data, that’s the problem. It could make life a lot more efficient, but we don’t have that trust, so we’re kind of stuck.’
Jurors felt that a centralised health data infrastructure presented many opportunities. The major benefits they saw were in improving responses to future public health emergencies, often through supporting the advancement of medical research:
‘I want this to be beneficial and work in the interests of medical research.’
‘I can also see there are huge benefits [from the GPDPR] for medical research.’
There was also a recognition of the potential for data in the GPDPR programme to help inform regional and local decision-making and planning.
Jurors felt that centralised data infrastructure represents an opportunity to improve the state of public health by analysing and responding to the intersection of socio-demographic factors with health. They noted that there was an independent process to review applications for access to data (the Independent Group Advising on the Release of Data – IGARD),19, and some jurors expressed their view that the oversight for access to data in place was ‘fairly robust’.
Risks of the GPDPR
Despite these oversight measures, jurors highlighted that their distrust of the Government posed a serious hindrance to realising the potential benefits of the GPDPR.
A strong concern related to how there was limited communication about the introduction of the GPDPR, and inadequate explanation of what options patients had to opt out of the scheme. Participants felt the acronym’s close parallel with GDPR was confusing and caused grounds for suspicion:
‘The fact that they chose the name GPDPR really undermined transparency.’
‘I’m furious about the acronym being so close to GDPR. That’s wrong. Everyone will assume that it is just GDPR and gloss over it and think, “I’m bored with it now”.’
Jurors suggested that there should be mechanisms to ‘keep people in the loop’ by informing them about the use of data:
‘If we are giving up our data, we need to be able to have a control of that and be able to see what others are seeing about us. That’s a level of mutual respect that needs to be around personal data sharing.’
Jurors also expressed concerns about the risks of potential third-party access to general practice data. They felt that there were risks of unfair profiteering from or misuse of NHS data by third parties, particularly commercial companies.20 Some jurors questioned the extent to which the NHS would benefit from the establishment of such infrastructure for third parties:
‘What is the NHS getting in exchange? I’m concerned it’s only pharmaceuticals that benefit from these arrangements.’
Jurors also raised questions about the relative costs of developing and maintaining a centralised infrastructure, and whether data security could be ensured. They were critical of the assumption that there is wide acceptance of the GPDPR and its benefits.
Conditions for good governance of the GPDPR
Jurors proposed several practical conditions for the good governance of the GPDPR:
- Policies, safeguards and accountability mechanisms to protect against exploitation and misuse of data by third parties, as well as to ensure that there is a fair exchange of NHS data that does not result in excessive profit.
- Provide more transparency, clear communication, and meaningful public and patient engagement.
- Mechanisms for active opt-in or informed consent – to address the perception that patients have limited or no control over the governance of their own data.
- Creating a publicly accessible registry of private companies using GPDPR, giving reasons for access and evidence of compliance.
- Measures to monitor and check how patient data was being used, in addition to publicly available audit trails of those applying to access data.
Vaccine passports, passes and certificates
As soon as the vaccine rollout began in autumn 2020 the UK Government – and many other governments around the world – began considering mechanisms to determine who had or had not been vaccinated. Such mechanisms have become known by various terms, such as vaccine passes, immunity certificates, COVID passes and more, but are most commonly referred to in the UK as vaccine passports. The Ada Lovelace Institute maintains a monitor of international developments of these systems, and has published several pieces of research on their ethical issues.21
In the citizens’ juries we used the term vaccine passports as a catch-all term for any mechanism to determine vaccination status, though jurors considered the nuances and variations in how different mechanisms might work. The jurors were introduced to a brief history of vaccine passports such as the smallpox passport, yellow pass for yellow fever and cholera and typhoid passports. They also heard from experts from UK-based research groups on the benefits, risks, challenges and concerns of vaccine passport schemes.
The jurors’ deliberations took place during a time of ongoing uncertainty about the role vaccine passports would play in the UK. As early as April 2020, the UK Government was considering implementing the use of vaccine passports in some form. Since then, vaccine passports have never been far from newspaper headlines or public debate, and a vaccine passport for international travel, the NHS COVID Pass, was first introduced in England on 17 May 2021.22 This pass has since been used in other settings, such as nightclubs and theatres, and on 8 December 2021, the UK government announced that COVID-19 status certification via the NHS COVID Pass would become mandatory for entry into nightclubs and other crowded or large venues as part of the ‘Plan B’ response to the Omicron variant.23 For a full history of developments around vaccine passports in the UK, see the Ada Lovelace Institute’s international monitor of vaccine passports and COVID-19 status apps.21
At the time of the deliberations, the NHS COVID Pass had been in operation for international travel for several weeks, though debate about what further role it would play was still ongoing. Below, we summarise jurors’ perspectives on the benefits, risks, and conditions for good governance of vaccine passports.
Benefits of vaccine passports
Jurors thought that vaccine passports could enable society to return ‘to normal’, for example by giving people greater confidence to interact in public spaces and allow hospitality and catering businesses to increase their capacity. They considered this to be the primary benefit offered by any vaccine passport scheme, but they also acknowledged the implications vaccine passports may have for individuals’ personal freedoms, privacy and liberties (discussed further below). When thinking about the balance of benefits and risks, some jurors took a utilitarian view: the ‘greatest good for the greatest number of people’
Jurors discussed other benefits too, including the possibility for vaccine passports to support public bodies to understand the efficacy of vaccine rollouts. Some highlighted the potential benefit to those who were most clinically vulnerable, for example by enabling them to participate in events and activities where they can be sure others present are vaccinated, and so less likely to spread infection.
With regards to international travel, jurors pointed out that not all travel involved leisure, and that vaccination passports might enable workers in the UK to visit family members and allow travel for business purposes. There was some interest and appetite specifically in an international or universal vaccine passport specifically for the purposes of travel for such reasons.
Risks of vaccine passports
‘Are vaccine passports a slippery slope that erodes liberties?’
Jurors expressed concern that vaccine passports could introduce ‘social grading’ by distinguishing between two classes of people (one vaccinated, and another unvaccinated), and might be the beginning of a ‘slippery slope’ towards a multi- or two-tiered society.
Many jurors described their concerns that vaccination passports, in distinguishing between those who were vaccinated and those who were not, are ‘discriminatory by design’ and risk perpetuating digital inequalities, including against those individuals who chose not to or were advised by medical professionals not to be vaccinated. Some jurors were concerned that those who were medically vulnerable or had lower immunity might well be at a greater risk of being discriminated against due to the implementation of vaccine passports.
‘I think these passports are discriminatory …I remember a certain millionaire who has a plumbing business in London was saying all of his employees had to be vaccinated to have a job with him.’
Jurors were particularly concerned about requiring proof of vaccination for essential aspects of daily life and expressed that evidence of vaccination or a negative COVID-19 test result must be proportionate to the context, balancing both necessity and risk. They felt that vaccine passports as a condition for employment creates unfair social divides and could incentivise demand for fraudulent proof of vaccination. Many jurors thought using vaccine passports is unnecessary and exclusionary for those who are not vaccinated in venues such as supermarkets where contact is limited and people do not spend as much time.
For some jurors, disproportionate use of vaccine passports, particularly where they may have limited impact on reducing infections, reinforced concerns about infringements of personal freedom and autonomy, undermining people’s free decision to be vaccinated or not.
Jurors also recognised that vaccine passports had limitations. Vaccinated people may still be infected and infectious, even if they can demonstrate their vaccination status. Moreover, jurors identified the potential risks associated with fraudulently misrepresenting vaccination status, or to acquire falsified proof of vaccination.
Other questions were raised about the interoperability of vaccine passports across international settings. Jurors questioned whether vaccine passports would always be effective for international travel when there is reliance on different countries’ standards for vaccine passports in addition to different standards for vaccination status. Given the UK NHS COVID Pass was not recognised in the EU until October 2021, the jurors’ discussions in July 2021 are remarkably prescient.25
Conditions for good governance of vaccine passports
Vaccine passports were a highly contested issue, and some jurors indicated that they would not feel comfortable with the use and implementation of vaccine passports in any circumstances.
Where some jurors felt there were grounds for implementation, specifically during the pandemic, they expected the following conditions as prerequisites for good governance:
- Published and clear public guidance on when vaccine passports are required and how they will be implemented.
- Support for businesses and other service providers in implementing vaccine passports by supplying the necessary digital infrastructure, as well as clear guidance around how to implement vaccine passport checks.
- Clear parameters for use, application and context. For example, specifying in which contexts and circumstances vaccine passports may be used.
- Engagement with citizens to include their perspectives in the design and evaluation of systems and tools involved in vaccine passports, for example the user-facing NHS COVID Pass app.
- Published and clear public guidance on when vaccine passports are required and how they will be implemented.
- Support for businesses and other service providers in implementing vaccine passports by supplying the necessary digital infrastructure, as well as clear guidance around how to implement vaccine passport checks.
- Clear parameters for use, application and context. For example, specifying in which contexts and circumstances vaccine passports may be used.
- Engagement with citizens to include their perspectives in the design and evaluation of systems and tools involved in vaccine passports, for example the user-facing NHS COVID Pass app.
- Regular reviews of the vaccine passport implementation, and transparent communication about the decision-making
- Strict and specific guarantees and safeguards in respect to the bounded use of vaccine passports, for example, to ensure that vaccination records are not shared with risk-scoring or social credit systems.
Data-driven risk scoring
The third case study considered by jurors included data-driven risk-scoring algorithms, such as the Oxford University QCovid model commissioned by the UK’s Chief Medical Officer Chris Whitty.26
This algorithm has been used to inform the NHS Digital Shielded Patient List, a list used to advise which people are clinically vulnerable to COVID-19 and should shield. Other uses of data-driven risk scoring include targeting healthcare resources and prioritising vaccine allocation.
Risk-scoring algorithms use data about patients’ existing health conditions and consider factors that contribute to patients’ risk levels, such as ethnicity and location deprivation data, to understand their vulnerability to COVID-19. When QCovid was used by NHS Digital in February 2021, it added an additional 1.7 million people to the national shielded patient list in February 2021 and prioritised them for vaccination.27
Although the Shielded Patients List was dismantled in September 2021, it was still active at the time of the jurors’ deliberations, and in January 2022 QCovid remained available for use by researchers and the NHS.28
Jurors wanted to consider risk-scoring algorithms given the vast amounts of data used by such systems, the digital infrastructure which underpins them, and the automated decision-making involved in the algorithms.
Benefits of data-driven risk scoring
Jurors felt that risk-scoring algorithms like QCovid had significant benefits for supporting the public health response to the pandemic. They were positive about how risk-scoring algorithms could reduce the pressure on the NHS by minimising the risk of hospitalisation for those who would be seriously affected, and by making vaccination more targeted and therefore effective at a population level.
Beyond immediate responses to COVID-19, jurors felt that the benefits of risk scoring included aiding medical teams to make better assessments of necessary interventions and generating community-specific medical and public health responses. They thought that in the long term, risk-scoring algorithms could generate data that complements community-led awareness and understanding of changing situations among vulnerable populations. Risk-scoring algorithms could also be used to identify and address non-medical risks or social determinants of wellbeing such as housing, financial situation or food poverty. Indeed, this is exactly how some local authorities began deploying these types of algorithms.29
Risks of risk-scoring algorithms
Jurors were concerned about how risk-scoring algorithms and the Shielded Patient List assigned a particular status to highly vulnerable people that might create the potential for errors, misuse or abuse. Some jurors queried whether risk scoring had the effect of stigmatising or shifting responsibility onto the ‘risky person’, rather than ensuring collective or Government accountability, and emphasised the importance of cautious use of risk-scoring algorithms, so that they did not have the effect of demonising people. Jurors discussed the potential for future scope creep or questionable applications in non-health contexts, for instance for criminal or financial purposes.
Jurors also expressed anxiety about how the uncritical reliance on risk scoring might adversely affect clinical and human decision-making. They questioned whether use of these algorithms might engender false confidence in the quality, reliability and fairness of their outputs:
‘My fear is that the control of these things will have no checks and measures because everyone will rely on them.’
Jurors wanted guarantees that the quantitative data used in the algorithm would be complemented with qualitative data and robust approaches to integrating the two in the ultimate risk assessments.
Conditions for good governance of data-driven risk scoring
Jurors’ views on data-driven risoring were less divided than those about vaccine passports, and there was more emphasis on ‘getting its use right’. However, it is important to note that their discussion remained confined to the parameters of the pandemic health response, rather than on use of risk-scoring algorithms beyond the pandemic.
The following were some conditions jurors proposed for good governance of data-driven rising during the pandemic:
- Human discretion on a risk-scoring algorithm’s decision for individualised advice, and ensuring those decisions are embedded within clinical and local decision-making infrastructures rather than imposed ‘top-down’.
- Sharing knowledge and learning across different parts of the UK while preserving local autonomy in putting information from risk scoring to best use.
- An auditing process that covers definitions of risk, data quality checks and process of accounting for, and amending errors emerging from the use of risk scoring.
- Improved communications and transparency about the functions, uses and future of risk scoring.
- A clear data governance framework that limits the use of risk-scoring assessment and data to medical services, treatments and research, and considers the appropriateness and quality of data available.
- Co-production and working closely with marginalised and underrepresented people in the use and governance of risk scoring.
- Society-based and community-based infrastructure to support those identified as vulnerable, ensuring that approaches benefit impacted communities, rather than demonise them.
Conclusion: red lines and principles for good data governance
During the final day of their deliberations, jurors discussed red lines that set the limits of acceptability for data-driven technologies used in response to pandemics.
Jurors’ red lines for data-driven technologies used in pandemics:
- Technologies should not create a two-tiered society. Jurors were concerned about applications of data-driven technologies that could lead to demonised, stigmatised or otherwise marginalised individuals or groups.
- Measures exceptionally and temporarily accepted during the pandemic should not be extended into the future. Jurors acknowledged that some exceptional measures were appropriate and justified in the emergency circumstances. However, they expect to see time and purpose limitations, or at the very least reassessment and review, to ensure those measures do not extend beyond those circumstances.
- Technologies should not be used to surveil, influence, profile or predict the behaviour of individuals. Jurors expressed significant discomfort across a range of case studies where individuals might be influenced for an illegitimate purpose through the use of technologies to behave in particular ways against their own free will.
These red lines, together with the 7 principles and participants’ perspectives represented in this report, articulate this group of citizens’ views on what the good governance of data must look like to gain public trust. These findings provide strong evidence for policymakers, public health officials and technology developers looking to ensure that measures responding to a pandemic are worthy of public trust.
However, the limits of these findings lie in the gap that persists between any set of principles and putting those principles into practice. But as the jurors’ views on the different case studies show, exactly how principles for good governance are applied in practice depends largely on the particular data-driven technology under consideration. One clear action policymakers and technologists can take in the future, then, is to conduct robust public engagement around any proposed data-driven intervention. This would be a first step towards ensuring public trust and good governance in the use of data during pandemics.
Methodology: citizens’ juries recruitment and structure
About citizens’ juries
A citizens’ jury is a type of structured deliberation with members of the public, sometimes referred to as a mini public.
First developed by the Jefferson Centre in the 1970s, citizens’ juries involve a demographically diverse sample of a population who act as the ‘jurors’ and participate in a series of meetings to consider information about an issue, develop informed opinions, and deliberate on solutions or conclusions.30 Citizens’ juries usually address issues of public policy, and the conclusions generated often take the form of recommendations for decision-makers in local or national government, or other public office.31
During citizens’ jury meetings, often called workshops, balanced information about the chosen issue is given to the jurors and expert witnesses give presentations drawing on their professional, academic or lived experience. Trained facilitators assist the jurors by structuring the workshops, guiding jurors through the agenda and facilitating dialogue with the expert witnesses.
Deliberative mini publics like citizens’ juries have several advantages. They empower citizens to develop informed opinions and make decisions about issues that affect them. For policymakers, these deliberations can help identify both barriers and solutions to public policy issues, such as building trust in government institutions as they deploy data-driven technologies.32 At times of crisis, citizen deliberation is an effective approach to public consultation that can contribute to lessening the democratic deficits of technological solutionism and technocracy.7
Our methodology
For this project we conducted two week-long citizens’ juries via Zoom in July 2021.34
The project involved 50 jurors in total, with 25 jurors participating in each week of deliberations. Jurors were recruited to reflect the demographic diversity of the UK population according to age, gender, ethnicity and region, and people who reported being clinically vulnerable to COVID-19 were deliberately overrepresented. The jurors were remunerated at best practice rates for their involvement in 10 hours’ deliberation each, and we worked with research agency PeopleForReseach to recruit them.35
We invited 13 expert witnesses to present to the jurors and five officials from NHSX (now part of the NHS Transformation Directorate),36 the Scottish Government and the Office for Statistics Regulation to listen to the jurors’ comments in the final session. There is a full list of experts and officials in the acknowledgements at the end of this report.
Jurors met for two-and-a-half hours each day from Monday to Thursday in a single week, to hear presentations and take part in facilitated discussions in breakout groups. Each jury followed the same structure:
| Day 1 | Jurors were introduced to the project, provided with an overview of data-driven technologies deployed in response to the pandemic, and given some initial provocations around challenges for the rule of law and good governance. |
| Days 2-3 | Jurors were given presentations about their chosen case studies – vaccine passports, risk-scoring algorithms and the General Practice Data for Planning and Research programme (GPDPR) – from experts who spoke either for or against each case study. |
| Day 4 | Jurors reflected on all they had heard in the previous days and discussed conclusions. |
Annex 1 presents a detailed summary of the structure of the citizens’ juries and lists the expert witnesses.
Using notes and transcripts from the workshops, we applied thematic analysis to group common topics and themes in the jurors’ perspectives.37 From this analysis, we developed the seven principles presented in this report, and throughout this report we describe the jurors’ perspectives according to these themes.
Other research methods often quantify responses (for example, ‘40% of participants said x’), but such descriptions do not accurately reflect the nature of public deliberation. Instead, in this report we use language such as ‘some jurors felt’ or ‘there were some concerns’ to describe perspectives raised throughout the dialogue, but which did not dominate or permeate through all topics. Where we use language such as ‘jurors felt’ or ‘there was a strong sense’, this indicates a finding that was prominent in the deliberations, received strong consensus, or was raised frequently by many participants.
Acknowledgements
The project is funded by the Arts and Humanities Research Council as part of the UK Research and Innovation rapid response to COVID-19.
This report was authored by Reema Patel, Aidan Peppin (Ada Lovelace Institute) and Nardine Alnemr (Centre for Deliberative Democracy and Global Governance, University of Canberra). The citizens’ juries were organised and project-managed by Kayshani Gibbon and Reema Patel, with lead facilitation also from Aidan Peppin and Dr Mavis Machirori (Ada Lovelace Institute).
We are grateful to Dr Claudia Pagliari (University of Edinburgh) and Dr Jan Van Zyl Smit and Dr Irene Pietropaoli (Bingham Centre for the Rule of Law) for advice, guidance and oversight of this report.
We thank the expert witnesses and advisers who contributed to the citizens’ juries. These include:
Professor Lilian Edwards, Newcastle University
Dr Jan van Zyl Smit, Bingham Centre for the Rule of Law
Dr Claudia Pagliari, University of Edinburgh
PeiChin Tay, Tony Blair Institute
Kirsty Innes, Tony Blair Institute
Phil Booth, MedConfidential
Jess Morley, University of Oxford
Dr Marion Gibbon, Birmingham City Council
Professor Jeremy Brown, University College London
Dr Natalie Banner, Understanding Patient Data
Cori Crider, Foxglove
Michael Chapman, NHS Digital
Brhmie Balaram,
Ed Humpherson, Office for Statistics Regulation
Doreen Grove, Scottish Government
Jennifer Berger, NHSX
Anjali Mazumder, The Alan Turing Institute
Imogen Parker, Ada Lovelace Institute
Carly Kind, Ada Lovelace Institute
All organisational affiliations correct at time of juries’ deliberations.
Our greatest thanks are reserved for the 50 jurors who each joined a week-long jury, contributing their time, efforts, and input to guide policymakers about good governance of data-driven technologies and post pandemic data futures.
Annex 1: Summary of the juries’ structure
| Date | Topics | Expert speakers |
| Jury 1, 12-15 July 2021 | ||
| 12/07/2021
Scene setting |
Introducing the project
Overview of data-driven technologies deployed in responses to the pandemic
Challenges for the rule of law
What is good governance? |
Reema Patel, Ada Lovelace Institute
Lilian Edwards, University of Newcastle
Jan van Zyl Smit, Bingham Centre for the Rule of Law
Claudia Pagliari, University of Edinburgh/Scottish Government’s National Expert Group in Digital Ethics |
| 13/07/2021
Exploring the use of vaccine passports |
Overview of vaccine passports
Arguments for vaccine passports
Arguments against vaccine passports |
Imogen Parker, Ada Lovelace Institute
PeiChin Tay, Tony Blair Institute
Phil Booth, MedConfidential |
| 14/07/2021
Exploring the use of risk scoring (QCovid)
|
Overview of risk scoring and GPDPR
Risk scoring, identification of vulnerable groups and limitations of the system
Opportunities in using risk scoring during the pandemic for reduced death and hospitalisation rates
|
Jess Morley, University of Oxford
Marion Gibbon, Birmingham City Council
Jeremy Brown, University College London |
| 15/07/2021
Reflections on good data governance during pandemics
|
Synthesising previous deliberations to discuss key insights with policymakers | Doreen Grove, Scottish Government
Jennifer Berger, NHSX |
| Jury 2, 19-22 July 2021 | ||
| 19/07/2021
Scene setting |
Introducing the project
Overview of data-driven technologies deployed in responses to the pandemic
Challenges for the rule of law
|
Reema Patel, Ada Lovelace Institute
Lilian Edwards, University of Newcastle
Jan van Zyl Smit, Bingham Centre for the Rule of Law
|
| 20/07/2021
Exploring the use of vaccine passports |
Overview of vaccine passports
Arguments for vaccine passports
Arguments against vaccine passports |
Imogen Parker, Ada Lovelace Institute
Kirsty Innes, Tony Blair Institute
Phil Booth, MedConfidential |
| 21/07/2021
Exploring the use of the GPDPR in the context of COVID-19
|
Overview of GPDPR
Evidence of discriminatory tech and lack of accountability
Benefits and opportunities in GPDPR |
Natalie Banner, Understanding Patient Data
Cori Crider, Foxglove
Michael Chapman, NHS Digital |
| 22/07/2021
Reflections on good data governance during pandemics
|
Synthesising previous deliberations to discuss key insights with policymakers |
Brhmie Balaram, NHSX
Ed Humpherson, Office for Statistics Regulation Anjali Mazumder, Alan Turing Institute
|
- Adapted from a presentation shown to jurors by Dr Claudia Pagliari during their workshops.
- The first is in reference to Dominic Cummings violation of lockdown restrictions in April 2020. The second reference is to a video of Number 10 officials ‘joking’ about rehearsing their response to inquiries about their Christmas party in 2020 despite the lockdown. More details about these two incidents are covered under the sub-heading ‘trustworthiness of Government, public institutions, technology developers and the private sector’.
- This was also a live consideration raised in a previous dialogue by the Ada Lovelace Institute and Traverse on contact tracing, see: Ada Lovelace Institute. (2020). Confidence in a Crisis? Building public trust in a contact tracing app. Available at: https://www.adalovelaceinstitute.org/report/confidence-in-crisis-building-public-trust-contact-tracing-app/
- McGee, L. (2021). ‘Boris Johnson’s aides joked about Christmas party in Downing Street while London was in lockdown’. CNN. Available at: https://edition.cnn.com/2021/12/08/uk/boris-johnson-christmas-party-2020-intl-gbr/index.html
- For a definition of ‘responsibilisation’, see: Wakefield, A. and Fleming, J. (2009). ‘Responsibilization’. The SAGE Dictionary of Policing. Available at: https://sk.sagepub.com/reference/the-sage-dictionary-of-policing/n111.xml
- Ada Lovelace Institute. (2020). Exit through the App Store?. Available at: https://www.adalovelaceinstitute.org/evidence-review/covid-19-rapid-evidence-review-exit-through-the-app-store/
- Patel, R. (2020). Why we cannot afford to leave technology to the experts – the case for public engagement at times of crisis. Ada Lovelace Institute. Available at: https://www.adalovelaceinstitute.org/blog/distrust-data-sharing-engage-deliberate-decide/
- Park, S. (2017). ‘Introduction’. Digital Capital. Available at: https://link.springer.com/chapter/10.1057/978-1-137-59332-0_1
- Ada Lovelace Institute. (2021). The Data Divide. Available at: https://www.adalovelaceinstitute.org/report/the-data-divide/
- ZOE is an app used to crowdsource COVID-19 and nutrition health data for the purposes of academic research. Data is also shared with the NHS and the Government. For more information, see: https://covid.joinzoe.com/
- See: Kennedy, H. et al. (2020). Public understanding and perceptions of data practices: a review of existing research. University of Sheffield. Available at: https://livingwithdata.org/project/wp-content/uploads/2020/05/living-with-data-2020-review-of-existing-research.pdf
- Serco is a private company, one of four contractors, operating 20% of the COVID-19 testing sites as part of the NHS ‘test and trace’ programme. High profits accrued by private contractors, such as Serco, during the pandemic received criticism from the public. See: Jolly, J. (2020). ‘Serco profits surge thanks to Covid-19 test-and-trace contract’. The Guardian. Available at: https://www.theguardian.com/business/2020/oct/16/serco-considering-dividend-payout-covid-test-and-trace-boosts-profits
- See: NHS Digital. (2021). General Practice Data for Planning and Research (GPDPR). Available at: https://digital.nhs.uk/data-and-information/data-collections-and-data-sets/data-collections/general-practice-data-for-planning-and-research
- See: Boiten, E. (2021). ‘NHS plan to share GP patient data postponed – but will new measures address concerns?’ The Conversation. Available at: https://theconversation.com/nhs-plan-to-share-gp-patient-data-postponed-but-will-new-measures-address-concerns-165103
- Crouch, H. (2021). ‘NHS Digital announces new primary care data collection service’. Digital Health Available at: https://www.digitalhealth.net/2021/05/nhs-digital-announces-new-primary-care-data-collection-service/
- This summary is based on the GPDPR overview delivered by Dr Natalie Banner from Understanding Patient Data at the citizens’ jury on 21 July 2021.
- NHS Digital. (2021). Improved collection of GP data launched. Available at: https://digital.nhs.uk/news/2021/improved-collection-of-gp-data-launched
- NHS Digital. (2021). GP Data for Planning and Research: Letter from Parliamentary Under Secretary of State for Health and Social Care to general practices in England. Available at: https://digital.nhs.uk/data-and-information/data-collections-and-data-sets/data-collections/general-practice-data-for-planning-and-research/secretary-of-state-letter-to-general-practice
- See: NHS Digital. (2021). Independent Group Advising on the Release of Data (IGARD). Available at: https://digital.nhs.uk/about-nhs-digital/corporate-information-and-documents/independent-group-advising-on-the-release-of-data
- For previous research on public attitudes to fair use of NHS data, see: Ada Lovelace Institute and Understanding Patient Data. (2020). Foundations of Fairness. Available at: https://www.adalovelaceinstitute.org/news/accountability-transparency-participation-third-party-use-nhs-data/
- Ada Lovelace Institute. (2021). International monitor: vaccine passports and COVID-19 status apps. Available at: https://www.adalovelaceinstitute.org/project/international-monitor-vaccine-passports-covid-status-apps/
- Ada Lovelace Institute. (2021).
- Nanu, M. and Hall, S. (2021). ‘Boris Johnson confirms return of working from home as England moves to Plan B’. The Telegraph. Available at: https://www.telegraph.co.uk/global-health/science-and-disease/covid-news-coronavirus-omicron-stealth-variant-cases-vaccine/
- Ada Lovelace Institute. (2021). International monitor: vaccine passports and COVID-19 status apps. Available at: https://www.adalovelaceinstitute.org/project/international-monitor-vaccine-passports-covid-status-apps/
- Lewis, J. (2021). ‘Can I use my NHS Covid Pass for travel?’. iNews. Available at: https://inews.co.uk/inews-lifestyle/travel/nhs-covid-pass-travel-can-use-when-eu-accept-uk-vaccine-passport-countries-take-now-1249765
- University of Oxford. (2021). Oxford-led technology to help those at high risk from COVID-19. Available at: https://www.ox.ac.uk/news/2021-02-16-oxford-led-technology-help-those-high-risk-covid-19
- QCovid Risk assessment. QCovid risk calculator. Available at: https://qcovid.org/
- NHS Digital. (2021). Shielded Patient List. Available at: https://digital.nhs.uk/coronavirus/shielded-patient-list
- Local Government Association. (2021). Using the UPRN to identify vulnerable individuals and provide support during the pandemic in Barnsley Council. Available at: https://www.local.gov.uk/case-studies/using-uprn-identify-vulnerable-individuals-and-provide-support-during-pandemic
- Center for New Democratic Processes. How We Work, Citizens Juries. Available at: https://www.cndp.us/about-us/how-we-work/
- For more on citizens’ juries, see: Gakhal, J. et al. (2020). ‘Method: Citizens’ Juries.’ Participedia. Available at: https://participedia.net/method/155; Smith, G. and Wales, C. (2000). ‘Citizens’ Juries and Deliberative Democracy’. Political Studies, 48, pp. 51–65. Available at: https://journals.sagepub.com/doi/10.1111/1467-9248.00250
- Machirori, M. and Patel, R. (2021). Turning distrust in data sharing into ‘engage, deliberate, decide’. Ada Lovelace Institute. Available at: https://www.adalovelaceinstitute.org/blog/distrust-data-sharing-engage-deliberate-decide/
- Patel, R. (2020). Why we cannot afford to leave technology to the experts – the case for public engagement at times of crisis. Ada Lovelace Institute. Available at: https://www.adalovelaceinstitute.org/blog/distrust-data-sharing-engage-deliberate-decide/
- See the Ada Lovelace Institute’s view on using Zoom as a video conferencing tool here: https://www.adalovelaceinstitute.org/digital-best-practices-policy/
- See: People for Research. Available at: http://www.peopleforresearch.com
- NHSX is now part of the NHS Transformation Directorate. More information is available at: https://www.nhsx.nhs.uk/blogs/nhsxmoves-on/ At the time of research and writing, NHSX was a joint unit of NHS England and the UK Department of Health and Social Care that reported directly to the Secretary of State and the Chief Executive of NHS England and NHS Improvement.
- Attride-Stirling, J. (2001). ‘Thematic networks: an analytic tool for qualitative research’. Qualitative research, 1(3), pp. 385–405.